PT
Classroom - A Review of Patellar Taping
for Patellofemoral Pain Syndrome
׀
by Chai Rasavong, MPT,
MBA
.
The patellofemoral joint is influenced
significantly by the quadriceps muscle (line of pull, strength),
shape of the trochlear sulcus, shape of the patella, surrounding
soft tissue, biomechanics at the hip and foot, position of the
tibiofemoral joint (quad insertion), pelvic obliquities/SI joint
dysfunction, leg length differences, lower extremity flexibility
and/or muscle imbalances (1).
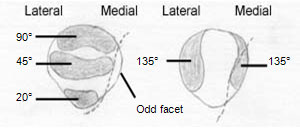
“Compressive forces begin at 20-30 degrees of flexion between the medial
and lateral facets of the patella and the femoral condyles. As
flexion continues, the patellar articular surfaces segmentally come
in contact with the trochlear groove with the exception of the odd
facet. Continuation of flexion allows a smaller portion of the
medial aspect of the patella to be contacted, with greater resultant
compressive force. With extreme flexion, the odd facet comes into
contact with the inner margin of the femoral condyle in the region
of the intercondylar groove (1). Below is an image displaying the
area where compressive forces are focused at the knee joint when
performing knee flexion”.
It is generally
believed that the alteration of patellofemoral kinematics can
contribute to patellofemoral pain syndrome. Individuals with
patellofemoral pain generally will have one of four patellar
malalignments. Please see article
“Understanding Patellofemoral
Dysfunction” by Kate Grace, PT, OPA-C & Annie Fonte, MBA” for
additional information.
Interventions for treating patellofemoral pain syndrome (PFPS) can
include patellar taping, patellar bracing, selective strengthening
of the vastus medialis muscle, stretching tight lateral structures,
correcting structural foot abnormalities, or a combination of these
interventions (2, 3, 4, 5). In this article we will review patellar
taping for the treatment of patellofemoral pain syndrome.
Patellar taping is sometimes utilized by physical therapists in
conjunction with other treatment interventions when treating
patients with PFPS. It is theorized that that most patients with
PFPS would benefit from medialization of the patella which would off
load the compressive forces at the lateral patellofemoral joint (2,
5). In a study by McConnell (5) she had a success rate of over 90%
when incorporating taping to correct for a glide, tilt and
rotational components of the patella along with emphasizing
closed-chain exercises. A study by Derasari et al (2) utilizing
dynamic magnetic resonance imaging revealed that taping resulted in
a significant patellofemoral inferior shift which may account for
some of the reported pain relief with taping, due to an increase in
contact area. In another study by Gilleard et al (4), they found
that taping the patellofemoral joint changes the onset of VMO and VL
activity. The earlier activation of the VMO may promote VMO activity
during retraining, improving patellar tracking.
Despite the positive findings in the above studies, other studies
concluded that although taping the patella medially can contribute
positively to PFPS rehabilitation, there were no significant changes
in patella positions (6, 7). A study by Gigante et al (6) utilizing
computed tomography found that patellar taping didn’t affect
patellofemoral lateralization or tilt, while another study by
Bockrath et al (3) utilizing Merchant’s view x-rays found no
significant changes occurring with patella rotation, patellofemoral
congruency, or sulcus angles. Although these studies didn’t reveal
significant changes in patella position with taping, their subjects
did demonstrate improvement with reduction of pain levels during
physical therapy related activities. These authors hypothesized that
the success of pain reduction from taping could be a result of
increase sensory input from the tape, enhanced support of the
patellofemoral ligaments and/or pain modulation via cutaneous
stimulation (3, 6, 7).
Although studies may vary as far as taping the patella to correct
for patella deviation, the majority of studies do concur that
patients did experience some sympotomatic relief with taping and
were able to better participate in physical therapy in order to
allow for more aggressive functional rehabilitation and to
facilitate compliance (2, 3, 4, 5, 6, 7).
Patella Taping Instructions (1)
1) Shave the area prn
2) Clean the area with alcohol prep
3) Position the patient in sitting with the knee in extension and
the quadriceps relaxed
4) Apply white pre-wrap (Hypafix). This extends from the lateral
epicondyle over the patella medially and posteriorly to the mid-popliteal
fossa.
5) Apply the brown rigid tape as indicated below (8)
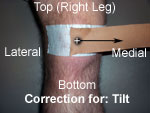
Lateral
tilt component is corrected by pulling the tape from the
midline of the patella medially.
Excessive
lateral tracking is corrected by pulling the patella medially.
Excessive
external rotation of the patella is corrected by taping from the
middle inferior patellar pole upward and medially.
An
anteriorposterior tilt of the patella is corrected by attempting to
tilt the inferior pole of the patella anteriorly by placing a strip
of tape at the superior pole of the patella and pulling the tape
medially.
6) Symptoms should decrease immediately upon application. If
present, always correct for AP (+) tilt first, then the worst
component next (1).
7) For tape removal, be sure to protect the skin. Peel of slowly and
hold the skin down. Tape remover may be necessary. Be especially
careful with patients who are elderly and/or who have frail skin.
Last revised: August 2, 2011
by Chai Rasavong, MPT, MBA
References
1. UW Madison PT 527 & 677. Foundations of Physical Therapy Practice / MSA &
T. Fall 1998 & Spring 2000.
2. Derasari A, et al. McConnell Taping Shifts the Patella Inferiorly in
Patients With Patellofemoral Pain: A Dynamic Magnetic Resonance Imaging
Study. Physical Therapy. 2010; 90(3):411-418.
3. Bockrath K, et al. Effects of Patella Taping on Patella Position and
Perceived Pain. Medicine and Science in Sports and Exercise. 1993;989-992.
4. Gilleard W, et al. The Effect of Patellar Taping on the Onset of Vastus
Medialis Obliquus and Vastus Lateralis Muscle Activity in Persons with
Patellofemoral Pain. Physical Therapy. 1998; 78(1):25-32.
5. McConnel J. The Management of Chondromalacia Patellae: A Long Term
Solution. The Australian Journal of Physiotherapy. 1986;32(4):215-223.
6. Gigante A, et al. The Effects of Patellar Taping on Patellofemoral
Incongruence: A Computed Tomography Study. Am J Sports Med. 2001;
29(1):88-92.
7. Christou E. Patellar taping increases vastus medialis oblique activity in
the presence of patellofemoral pain. J Electromyogr Kinesiol. 2004;
14(4):495-504.
8. Andrews J, Harrelson G, Wilk K. Physical Rehabilitation of the Injured
Athlete. Second Edition. W.B. Saunders Company. 1998;384.388.
Please review our terms and conditions
carefully before utilization of the Site. The information on this Site is for
informational purposes only and should in no way replace a conventional visit to
an actual live physical therapist or other healthcare professional. It is
recommended that you seek professional and medical advise from your physical
therapist or physician prior to any form of self treatment.
Copyright 2005-2022 CyberPT Inc. All rights reserved.


 Lateral
tilt component is corrected by pulling the tape from the
midline of the patella medially.
Lateral
tilt component is corrected by pulling the tape from the
midline of the patella medially.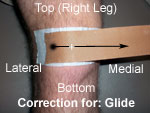 Excessive
lateral tracking is corrected by pulling the patella medially.
Excessive
lateral tracking is corrected by pulling the patella medially. Excessive
external rotation of the patella is corrected by taping from the
middle inferior patellar pole upward and medially.
Excessive
external rotation of the patella is corrected by taping from the
middle inferior patellar pole upward and medially.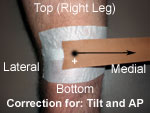 An
anteriorposterior tilt of the patella is corrected by attempting to
tilt the inferior pole of the patella anteriorly by placing a strip
of tape at the superior pole of the patella and pulling the tape
medially.
An
anteriorposterior tilt of the patella is corrected by attempting to
tilt the inferior pole of the patella anteriorly by placing a strip
of tape at the superior pole of the patella and pulling the tape
medially.





